This publication offers some ideas for drug treatment and harm reduction services keen to help people reduce smoking and tobacco-related harm. Its companion publication, Smoking among people facing problems with drug use, addresses the scale and impact of tobacco-related morbidity and mortality in this community.
There will be significant variations in what is applicable and achievable in different countries and contexts. Please adapt for local circumstances, taking what is useful for your staff and clients.
For more in-depth knowledge, our free online course, Understanding tobacco harm reduction, can be completed in two to three hours.
Key takeaways:
- Tobacco harm reduction is harm reduction – and harm reduction works.
- Smoking is the main cause of tobacco-related morbidity and mortality.
- Half of all who smoke long-term die prematurely from smoking-related diseases.
- Smoking rates are two to four times higher among people who use drugs than in the general population.
- Many people who use drugs suffer ill-health or premature death from smoking-related diseases.
- Nicotine does not cause cancer or COPD.
- Use of any non-combustible nicotine and tobacco products, especially where regulated, is safer than continued smoking. This includes nicotine vapes (e-cigarettes), nicotine pouches, Swedish snus and heated tobacco products.
- Misinformation means many people who smoke, and some health professionals, may be unaware that these products are much safer.
- Ignoring smoking is a missed opportunity to significantly improve clients’ health.
- Many people know smoking is harmful and want to stop or cut down; tobacco harm reduction empowers people to make choices that improve their health.
- Smoking cessation is linked to more positive long-term outcomes for people seeking to regain control over their use of, or dependency on, other substances.
- Smoking cessation is linked to better treatment outcomes for health conditions that disproportionately affect this group.
- Using safer nicotine products in tobacco harm reduction can be a low-cost, high-impact intervention for drug treatment and harm reduction services.
1. Introduction to tobacco harm reduction
1.1 What is tobacco harm reduction and why is it needed?
- Tobacco harm reduction is guided by the same principles as all other harm reduction approaches. It reduces the negative health impacts of tobacco use by giving people the choice of much safer nicotine products.
- Globally, most tobacco users smoke cigarettes. Cigarettes are the most dangerous way of consuming tobacco.
- All other smoked products (e.g. rolled tobacco, bidis, cigarillos, hookah, pipes, cigars) are also very risky to health. Some smokeless tobaccos (e.g. betel quid, paan, gutkha) also carry high risk.
- Smoking is the primary cause of tobacco-related morbidity and mortality. Half of all who smoke long-term die prematurely from smoking-related diseases.[1]
- People smoke to use nicotine, a relatively low-risk but dependence-forming stimulant released when tobacco burns. Burning tobacco releases approximately 7,000 chemicals, 70 of which are known carcinogens.[2]
- Nicotine does not cause cancer, COPD or other common tobacco-related illnesses; it is on the WHO List of Essential Medicines in the form of Nicotine Replacement Therapy (NRT).[3]
1.2 What are safer nicotine products and how do they work?
- Safer nicotine products include nicotine vapes, nicotine pouches, snus and heated tobacco products. All deliver nicotine without burning tobacco, reducing exposure to the multiple toxicants and carcinogens present in tobacco smoke.
- Nicotine vapes (e-cigarettes) use a battery to heat a coil or atomiser, turning a liquid containing nicotine and flavourings into a vapour that the user inhales.
- Swedish-style snus is sold mainly in small sachets which contain pasteurised ground tobacco and flavourings. Placed under the upper lip, nicotine is absorbed through the oral mucous membrane.
- Nicotine pouches are also small sachets, but instead of tobacco, they contain vegetable fibres infused with nicotine and flavours. These are also placed under the upper lip for nicotine absorption via the oral mucous membrane.
- Heated tobacco products use a battery to heat sticks of tobacco to no more than 350°C, below the level of combustion, which releases nicotine in a vapour that the user inhales.
1.3 Choosing products further down the scale of risk
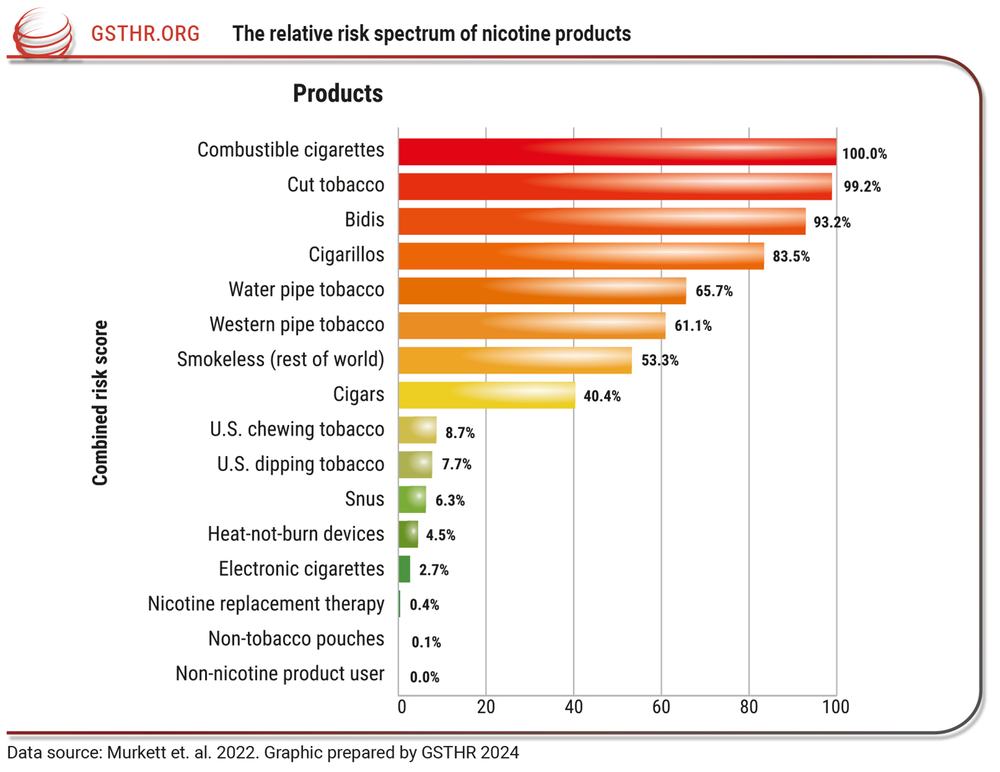
- A systematic review drew on 123 scientific studies to rank different nicotine products according to their risk profile for cancer and non-cancer tobacco-related diseases. The highest risk product, combustible cigarettes, was placed at 100%, with the risk facing a non-nicotine user at 0%. In comparison to cigarettes, the risk profile for all safer nicotine products ranked dramatically lower (see Figure 1).[4]
- To date, nicotine vaping’s positive role in smoking cessation has the largest evidence base, but evidence for other products is growing.
- Since 2012, an ongoing research review from Cochrane, considered the gold-standard in evidence-based medicine, has consistently found that nicotine vaping helps people to quit smoking and is more effective than NRT.[5]
- In 2023, the UK Government announced a world-first ‘Swap to Stop’ scheme, funding one million vape starter kits to help drive smoking rates down further.[6]
- The use of any non-combustible nicotine and tobacco products, especially where regulated, is safer than continued smoking.[7] While regulatory systems have developed in many countries, there remain many countries where safer nicotine products are not regulated, and some where they may be banned.
- Despite this, safer nicotine products are still available in most countries. While it cannot be guaranteed, it is likely that even unregulated products will be safer than continued smoking.
- The Global State of Tobacco Harm Reduction (GSTHR) estimates that around 200 million people worldwide are already using safer nicotine products.
- In numerous countries – Iceland, Japan, New Zealand, Norway, Sweden, the UK, the US – consumer uptake of safer nicotine products has been accompanied by an accelerated decline in smoking rates.[8]
- When available, accessible and affordable, many people will choose safer alternatives over continued smoking.
Figure 1
2. Tobacco harm reduction for people who face problems with their drug use
2.1 Smoking among people in contact with drug treatment
- A systematic review of 54 studies, covering over 37,000 people from 20 countries across six continents, showed that smoking rates among people in contact with drug treatment services were consistently two to four times higher than in the general population; the average smoking rate for people receiving opiate maintenance therapy was 85%.[9]
- A recent study of mortality data (2000–2018) for over 100,000 people who used heroin in England showed 63% died before the age of 70, compared to 16% of the general population.[10]
- Analysis of this data showed that tobacco smoking and illicit drugs each accounted for approximately one quarter of premature deaths among people who use heroin. Illicit drugs caused 28% of these deaths – but smoking accounted for 24%.[11]
- Supporting someone to reduce, manage or stop drug use, but not addressing their smoking, leaves them vulnerable to significant health risks and premature death.
2.2 Tobacco harm reduction in drug treatment: an opportunity for lasting change
- Desire to quit smoking is high among this population. Studies show between 50–80% of drug treatment clients report they are motivated to give up smoking.[12][13]
- It is a misconception that addressing smoking during drug treatment threatens people’s ability to regain control of their substance use. In fact, providing smoking cessation support reduces smoking rates and has either a neutral or positive effect on the outcomes of drug treatment.[14][15]
- Switching from smoking to safer alternatives has a positive impact on clients’ health and that of those around them; it reduces the risks of second-hand smoke for clients’ children and families, as well as for other clients and staff at support services, and decreases the risk of fires.
- Many people use safer nicotine products to reduce the number of cigarettes they smoke. This may be for the short-term, or it may be long-term. It is sometimes referred to as ‘dual use’. It also counts as harm reduction.
3. Integrating tobacco harm reduction into drug treatment and harm reduction services: practical approaches
This paper offers some ideas for how services could integrate tobacco harm reduction for their clients. It is important to acknowledge that there will be significant variations in what is applicable and achievable in different countries and contexts. Factors such as service resource, regulatory environments, product availability and cost will all vary. Please take what is useful for your staff and clients, adapting for local circumstances.
3.1 Lay the groundwork: what resources do you have available?
- Ascertain which safer nicotine products are available locally, investigating their regulatory status, accessibility and cost compared to continued smoking. The GSTHR’s free Global THR Database provides country-by-country information on the regulatory status of all safer nicotine products and NRT. Our research shows that at least one category of safer nicotine product is legally available in 128 countries.[16]
- Assess capacity and resourcing for in-house interventions. Many options cost nothing or very little, such as providing information on the health risks of smoking and safer alternatives, in conversations with clients and in printed materials in the service. If funded to do so, services could train staff to deliver cessation and switching support or supply safer nicotine products or vouchers for reputable vendors.
- Research relevant support nearby – if there are smoking cessation services, request their help; staff training or direct support for clients may be available.
- If no smoking cessation services operate nearby, support staff to receive specialist cessation training if possible. If local training is unavailable, the UK’s National Centre for Smoking Cessation and Training (NCSCT) offers free, open access online training.[17]
- Reputable local suppliers of safer nicotine products can also be a useful source of information and advice.
3.2 Introduce tobacco harm reduction to the service
- Assess staff attitudes to smoking, nicotine use and tobacco harm reduction, including their own use of tobacco and nicotine.
- Make staff aware of the high rates of smoking-related illness and premature death among drug treatment clients, highlighting that, in some circumstances, tobacco use may be more of a risk to their health than illicit drug use.
- Although sometimes seen as a way to bond or build trust, when staff smoke with clients, tobacco use is being reinforced and legitimised. This should be discouraged.
- Introduce the key concepts of tobacco harm reduction. Support staff to complete Understanding tobacco harm reduction, our free online course.
- Conduct baseline assessments with all existing and new clients, gathering data on tobacco and nicotine use and attitudes towards cessation.
- Encourage clients and staff to work together to reduce their smoking and quit or switch to safer nicotine products. Switching alongside one another offers new opportunities for fostering positive client/staff relationships.
- Create a cessation community in the service with shared goals, establishing a regular peer support group for clients and staff.
- Being able to see staff using safer nicotine products instead of cigarettes helps clients know that transition away from smoking is possible.
- Inform partner organisations and stakeholders – healthcare professionals, prescribing pharmacists, social workers – about the adoption of tobacco harm reduction. Ensure they are aware of the approach and the service’s aim to help people quit, reduce and/or switch away from smoking.
- Make decisions about use of safer nicotine products onsite/in dedicated spaces. People switching to safer products need somewhere to use their preferred options, separate from any dedicated smoking areas, to help avoid relapse.
- Display information and advice on safer nicotine use within the service. Provide clear signage on smokefree/safer product-friendly zones.
3.3 Equip staff with the confidence to tackle smoking through harm reduction
- Ensure staff are confident with the concepts of tobacco harm reduction. Use local resources where available alongside our free course, Understanding tobacco harm reduction, which offers deeper knowledge of the approach in just two to three hours of self-guided study.
- Support staff to deliver Very Brief Advice (VBA) with clients, a structured, concise intervention which can be delivered in less than one minute. VBA encourages clients to consider quitting, with professionals following these steps:
Ask whether they smoke;
Advise them to quit or switch;
Assess their interest in doing so;
Assist by providing information and advice to help quit or switch.
- The NCSCT’s Very Brief Advice on Smoking – 30 seconds to save a life provides more information and a clear flowchart to guide conversations.[18]
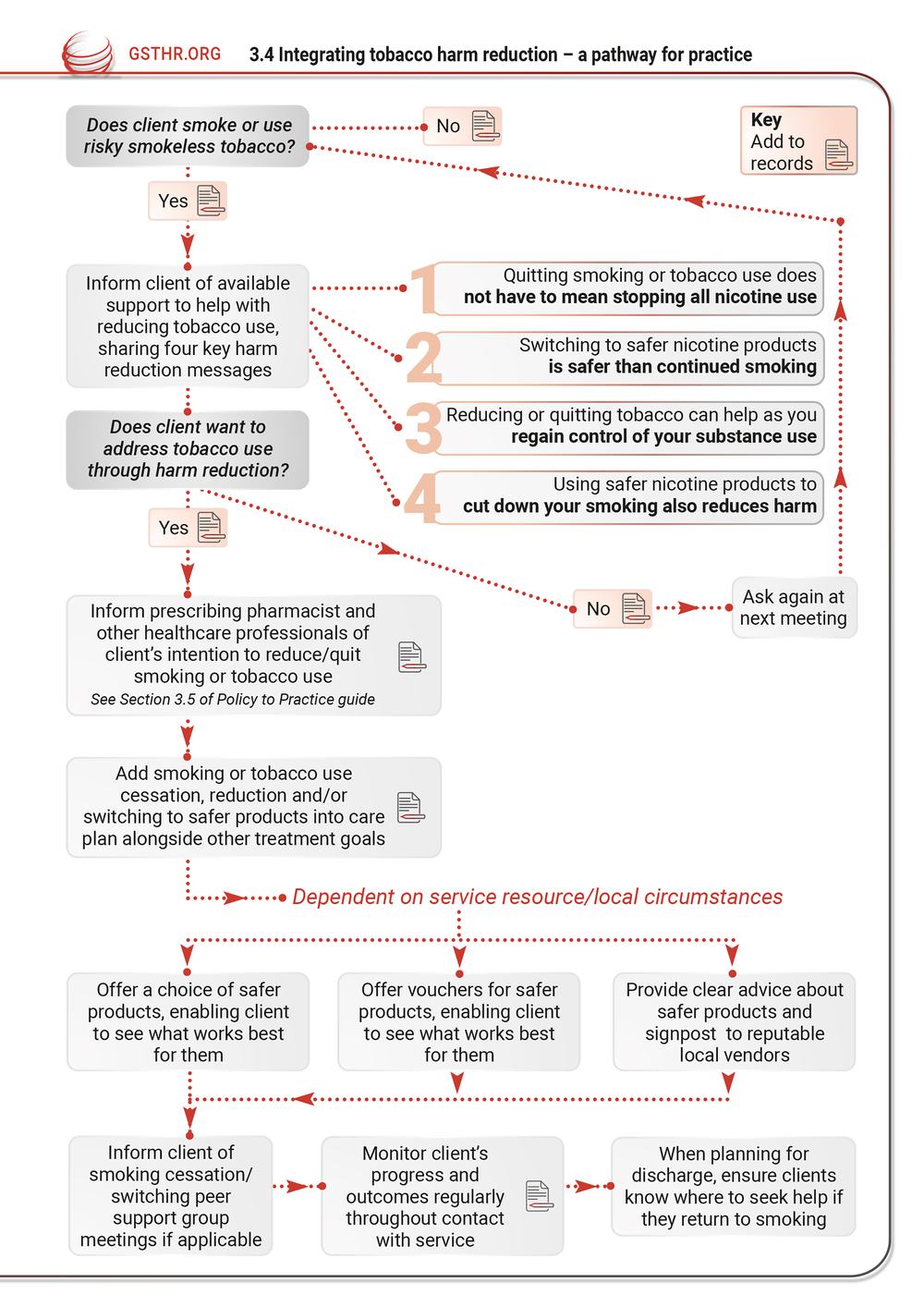
3.4 Integrating tobacco harm reduction – a pathway for practice
Figure 2
3.5 Safety considerations
- Smoking and/or nicotine use may interact with both prescribed and non-prescribed drugs used by clients. Smoking (not nicotine) can affect how the body metabolises some common medications, including methadone and several others likely to be prescribed to clients in drug treatment.[19]
- It is important to note that any risk associated with medication and changes to smoking and/or nicotine use will likely be minor compared to the significant health benefits of reducing or stopping smoking.
- Staff should refer to local prescribing guidance or seek advice from healthcare professionals who support or advise the service. Clear information can be found via the UK’s National Institute for Health and Care Excellence, Clinical Knowledge Summary: Which drugs are affected by stopping smoking? and Drug interactions – nicotine.
- Where appropriate, other healthcare professionals should be informed that clients are reducing or stopping smoking.
3.6 Monitoring and evaluation for long-term success
- Ensure information is collected on clients’ smoking or tobacco use, and desire/intention to quit or reduce, from first contact with the service.
- Monitor progress at regular intervals, collecting data on uptake of safer nicotine products and reduction and/or cessation of tobacco use.
- Gather both quantitative and qualitative data from clients and staff regularly as tobacco harm reduction is integrated into the service.
- Analyse data to evaluate the interventions and their outcomes, support ongoing improvements, demonstrate value and attract funding and resources.
4. Reducing tobacco harms, improving health
- Addressing high rates of smoking is essential to improve overall health for people in contact with drug treatment or harm reduction services.
- People in contact with these services smoke at higher rates than almost any other community. They are likely to have been smoking longer and find it harder to quit nicotine completely.
- Switching to safer nicotine products such as vapes, pouches, Swedish-style snus or heated tobacco products is safer than continued smoking.
- Many people know smoking is harmful and want to quit or cut down; tobacco harm reduction empowers people to make choices that improve their health.
- Stopping smoking does not have to mean abstinence from nicotine, if people cannot or do not want to stop. Switching to safer nicotine products offers people another route. And using safer nicotine products to reduce the number of cigarettes smoked is still harm reduction.
- Tobacco harm reduction does not have to cost services anything aside from time. The provision of information and guidance from a trusted source will reassure and empower clients to switch and find their preferred safer choice.
- Ignoring smoking is a missed opportunity to significantly improve clients’ health. Something is better than nothing. Whether the service can offer information, advice and signposting, or has the capacity to offer product starter kits, all actions are valuable and all have the potential to improve long-term health outcomes – for both clients and staff.
- Ultimately, tobacco harm reduction is harm reduction. And harm reduction works.
Resources / further reading
GSTHR Briefing Paper: Smoking among people facing problems with drug use
Companion publication addressing the scale of the smoking-related morbidity and mortality in this population.
Knowledge•Action•Change, UK. 2026.
Understanding tobacco harm reduction
Free online course, designed to be completed in 2–3 hours. Provides a foundation in tobacco harm reduction concepts.
Knowledge•Action•Change, UK. 2025.
GSTHR’s free database maps all aspects of safer nicotine product use and regulation, as well as smoking data and NRT availability.
Knowledge•Action•Change, UK. 2025.
GSTHR Briefing Paper: What is tobacco harm reduction? (2026 edition)
A detailed introduction to the principles, history and evidence for this vital public health strategy. Available in 13 languages.
Knowledge•Action•Change, UK. 2026.
GSTHR Briefing Paper: Why is tobacco harm reduction needed and what is the evidence it works?
Explains the importance of tobacco harm reduction and offers country case studies demonstrating the power of safer nicotine products to bring down rates of smoking. Available in 13 languages.
Knowledge•Action•Change, UK. 2025.
Addressing common myths about vaping
A short paper from Action on Smoking and Health (ASH) UK directly addressing some of the misinformation about nicotine vaping.
ASH, UK. 2023.
Very Brief Advice on Smoking – 30 seconds to save a life
Clear guidance on how to deliver this simple, fast intervention, including a flowchart to support conversations.
National Centre for Smoking Cessation and Training (NCSCT), UK. (2021).
The Smoking and Recovery Toolkit
Developed by US-based drug treatment practitioner John De Miranda as part of his participation in K•A•C’s Tobacco Harm Reduction Scholarship Programme, the toolkit offers resources on tobacco harm reduction for drug treatment services.
John de Miranda, US. (2021).
Clinical Knowledge Summary: Which drugs are affected by stopping smoking?
Clear information for potential impacts on prescribed medication for those reducing or stopping smoking.
National Institute for Health and Care Excellence, UK. (2025).
Website for checking common drug interactions. 94 drugs interact with nicotine: of the total drug interactions, 82 are moderate and 12 are minor.
Drugs.com. (Accessed March 2026).
For further information about the Global State of Tobacco Harm Reduction’s work, or the points raised in this GSTHR Briefing Paper, please contact [email protected]
About us: Knowledge•Action•Change (K•A•C) promotes harm reduction as a key public health strategy grounded in human rights. The team has over forty years of experience of harm reduction work in drug use, HIV, smoking, sexual health, and prisons. K•A•C runs the Global State of Tobacco Harm Reduction (GSTHR) which maps the development of tobacco harm reduction and the use, availability and regulatory responses to safer nicotine products, as well as smoking prevalence and related mortality, in over 200 countries and regions around the world. For all publications and live data, visit https://gsthr.org
Our funding: The GSTHR project is produced with the help of a grant from Global Action to End Smoking (formerly known as the Foundation for a Smoke-Free World), an independent, US non-profit 501(c)(3) grant-making organisation, accelerating science-based efforts worldwide to end the smoking epidemic. Global Action played no role in designing, implementing, data analysis, or interpretation of this Briefing Paper. The contents, selection, and presentation of facts, as well as any opinions expressed, are the sole responsibility of the authors and should not be regarded as reflecting the positions of Global Action to End Smoking.
[1] Tobacco. (2025, June 25). World Health Organization. https://www.who.int/news-room/fact-sheets/detail/tobacco.
[2] Center for Tobacco Products. (2026). Chemicals in Cigarettes: From Plant to Product to Puff. FDA. https://www.fda.gov/tobacco-products/products-ingredients-components/chemicals-cigarettes-plant-product-puff.
[3] eEML - Electronic Essential Medicines List. (n.d.). Retrieved 4 February 2026, from https://list.essentialmeds.org/recommendations/1097.
[4] Murkett, R., Rugh, M., & Ding, B. (2022). Nicotine products relative risk assessment: An updated systematic review and meta-analysis (9:1225). F1000Research. https://doi.org/10.12688/f1000research.26762.2.
[5] Lindson, N., Livingstone-Banks, J., Butler, A. R., McRobbie, H., Bullen, C. R., Hajek, P., Wu, A. D., Begh, R., Theodoulou, A., Notley, C., Rigotti, N. A., Turner, T., Fanshawe, T., & Hartmann-Boyce, J. (2025). Electronic cigarettes for smoking cessation. Cochrane Database of Systematic Reviews, 2025(11). https://doi.org/10.1002/14651858.CD010216.pub10.
[6] Smokers urged to swap cigarettes for vapes in world first scheme. (2023, April 11). GOV.UK. https://www.gov.uk/government/news/smokers-urged-to-swap-cigarettes-for-vapes-in-world-first-scheme.
[7] Murkett, R., Rugh, M., & Ding, B. (2022). Nicotine products relative risk assessment: An updated systematic review and meta-analysis (9:1225). F1000Research. https://doi.org/10.12688/f1000research.26762.2.
[8] Shapiro, H., Jerzyński, T., Mzhavanadze, G., & Porritt, O. (2024). The Global State of Tobacco Harm Reduction 2024: A Situation Report (No. 4; GSTHR Major Reports). Global State of Tobacco Harm Reduction (GSTHR). https://gsthr.org/resources/thr-reports/the-global-state-of-tobacco-harm-reduction-2024-a-situation-report/.
[9] Guydish, J., Passalacqua, E., Pagano, A., Martínez, C., Le, T., Chun, J., Tajima, B., Docto, L., Garina, D., & Delucchi, K. (2016). An international systematic review of smoking prevalence in addiction treatment. Addiction, 111(2), 220–230. https://doi.org/10.1111/add.13099.
[10] Lewer, D., Tattan-Birch, H., & Cox, S. (2025). Among people who use heroin, tobacco smoking and illegal drugs cause a similar number of premature deaths. Addiction, 120(12), 2573–2579. https://doi.org/10.1111/add.70140.
[11] Lewer, Tattan-Birch, & Cox, 2025.
[12] Syan, S. K., Belisario, K. L., Rahman, L., Levitt, E. E., McCarron, C., Radman, H., Amlung, M., Praecht, A., George, T. P., & MacKillop, J. (2025). Smoking in Substance Use Disorder Patients: Prevalence, Comorbidities, Impulsivity, and Patterns of Readiness to Change. Nicotine & Tobacco Research: Official Journal of the Society for Research on Nicotine and Tobacco, 27(10), 1813–1822. https://doi.org/10.1093/ntr/ntaf089.
[13] Cookson, C., Strang, J., Ratschen, E., Sutherland, G., Finch, E., & McNeill, A. (2014). Smoking and its treatment in addiction services: Clients’ and staff behaviour and attitudes. BMC Health Services Research, 14, 304. https://doi.org/10.1186/1472-6963-14-304.
[14] Apollonio, D., Philipps, R., & Bero, L. (2016). Interventions for tobacco use cessation in people in treatment for or recovery from substance use disorders. The Cochrane Database of Systematic Reviews, 11(11), CD010274. https://doi.org/10.1002/14651858.CD010274.pub2.
[15] Prochaska, J. J., Delucchi, K., & Hall, S. M. (2004). A meta-analysis of smoking cessation interventions with individuals in substance abuse treatment or recovery. Journal of Consulting and Clinical Psychology, 72(6), 1144–1156. https://doi.org/10.1037/0022-006X.72.6.1144.
[16] Knowledge·Action·Change. Global State of Tobacco Harm Reduction 2026. Forthcoming.
[17] Free stop smoking practitioner training and assessment. (n.d.). NCSCT E-Learning. Retrieved 25 March 2026, from https://elearning.ncsct.co.uk/free.
[18] Very Brief Advice on Smoking (VBA)+. (n.d.). National Centre for Smoking Cessation and Training. Retrieved 25 March 2026, from https://www.ncsct.co.uk/publications/VBA_2021.
[19] NICE. (2025, September 16). Clinical Knowledge Summary: Which drugs are affected by stopping smoking? The National Institute for Health and Care Excellence; NICE. https://cks.nice.org.uk/topics/smoking-cessation/ prescribing-information/drugs-affected-by-smoking-cessation/.