The paper is available for download (PDF) in following languages:
English Arabic Chinese (Mandarin) French German Hindi Indonesian Japanese Polish Portuguese Russian Spanish SwahiliKey concepts
Tobacco harm reduction is a potentially life-saving intervention for millions of people across the world. To those who currently use high-risk tobacco products, like cigarettes and some oral tobaccos, it offers the chance to switch to a range of safer nicotine products (SNP) that pose fewer risks to their health. And, while it is a relatively new addition to the arsenal of global public health solutions, its effectiveness builds on decades of success with earlier harm reduction initiatives.
Everyone uses products or behaves in ways that pose risks to our health. Governments do not try to stop people from driving, for example. What they do instead is enact laws about seat belt use and issue safety standards for manufacturers. These things reduce – but do not eliminate – the risk of injury or death.
In public health, harm reduction reduces health risks by providing people with safer alternative products and/or encouraging less risky behaviours, rather than by banning those products or behaviours. It emerged in the fight against HIV/AIDS in the 1980s and has since developed into a range of evidence-based, humane and cost-effective practices that save countless lives worldwide.
Most people know that tobacco use is harmful to health and that people use tobacco to consume nicotine. It is less well known that nicotine itself does not cause the severe illnesses associated with high-risk tobacco products like cigarettes. Nicotine is a comparatively low-risk drug, but its effects encourage repeated use. This is one of the reasons people find it hard to stop smoking, even when they know it is bad for their health.
The most dangerous way of using nicotine is by burning a cigarette and inhaling the smoke. Burning tobacco releases tar and gases containing thousands of toxins, many of which pose a risk of severe illness, leading to premature death in half of all smokers. Some oral tobacco products also release dangerous toxins when consumed.
In contrast, safer nicotine products (SNP) are non-combustible: none of them burn tobacco and some of them do not contain any tobacco at all. They include nicotine vapes (e-cigarettes), tobacco-free nicotine pouches, Swedish-style snus (an oral tobacco), many US smokeless (chewing) tobaccos and heated tobacco products. Many of these products have only been developed in the last 10 – 15 years.
Patches and gums represent another category of tobacco harm reduction product called nicotine replacement therapy (NRT). NRT and pharmaceutical products like varenicline (also called Champix) are effective for many people, while for others, they do not work. In many low and middle-income countries (LMIC), they are inaccessible or unaffordable.
SNP provide another option for people who want to reduce the harm connected to their use of nicotine. Many consumers report that they like vaping, using nicotine pouches, snus or heated tobacco products as they offer a more satisfying replacement for some of the habits and behaviours of smoking compared with other methods of quitting smoking.
Why is tobacco harm reduction needed?
Current efforts to curb smoking are not working quickly or effectively enough.
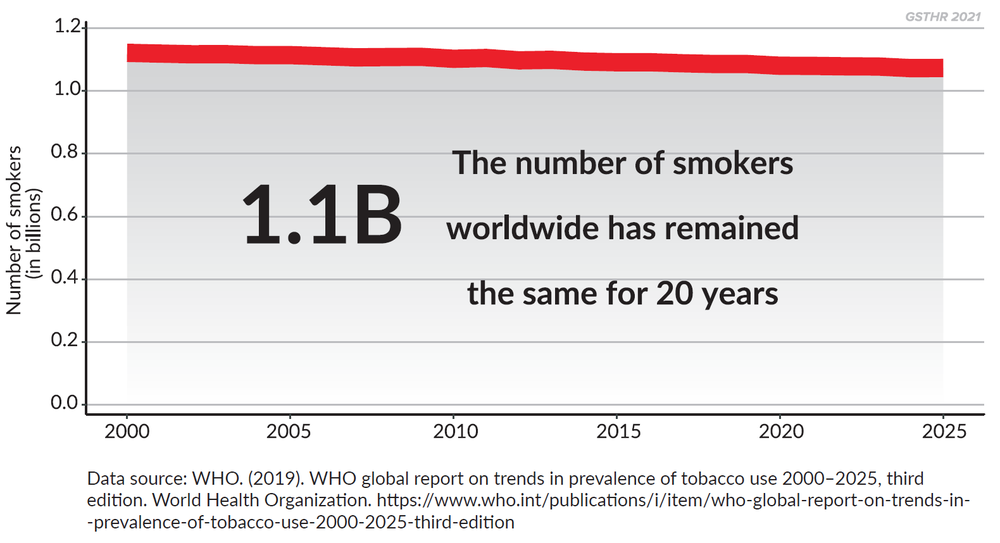
There are 1.1 billion smokers around the world, a figure that has remained unchanged since 2000, and 80 per cent of them live in LMIC. Many millions of people also use other risky tobacco products. The WHO’s projected death toll from smoking has not changed in 20 years and still stands at one billion by the end of the century. In 2006, the WHO forecast there would be 8 million deaths a year by 2030.[i] We are already there.
Current tobacco control measures are failing to reduce the death and disease caused by smoking.
Harm reduction history
Rather than coming from experts, harm reduction is often initiated by people who are directly affected by, or engaging in, risky behaviours, as a means of supporting their peers. Its development can be an organic and dynamic process.
When harm reduction first took off in the 1980s, communities were responding to the emergence of HIV among men who have sex with men, sex workers and people who inject drugs. People distributed condoms, sterile injecting equipment and advice on how to reduce the risk of contracting the virus. Initially these groups received no government help. The reaction of politicians, the media, society at large and many in the health sector was often hostile.
But by the late 1980s, politicians and the medical community in the UK began to recognise the potential benefits and cost-effectiveness of a harm reduction approach. This resulted in the UK’s success in limiting the spread of HIV. Other countries also saw steep falls in infection rates once they adopted harm reduction measures. Harm reduction works.
Harm reduction is particularly relevant to the use of psychoactive substances (those substances that alter your mental state). The use of mood-affecting products is common to all cultures and parts of the world with examples including caffeine, tea, nicotine, alcohol, cannabis, opium, tranquillisers, and psychoactive plants. Some substances are risky in themselves. For others, much of the risk lies in the way the drug is administered. For nicotine, the route of administration is crucial to the level of risk.
Is continued use of nicotine a concern?
Nicotine is on the World Health Organization’s list of Essential Medicines because medical practitioners have been prescribing nicotine patches and gums to people trying to quit smoking for decades.
The impact of nicotine on the brain is to encourage regular consumption, but it is a relatively low-risk substance and does not cause any of the health problems caused by cigarette smoke. The word ‘addiction’ conjures up the worst images of chronic alcohol and other drug use. This is misleading. Addiction is generally defined as compulsive use plus harm to self or others. Take away the harm and what is left is a compulsion to use a mild stimulant, similar to the use of caffeine.[ii]
How did tobacco harm reduction develop?
The idea of tobacco harm reduction can be traced to the British tobacco researcher Michael Russell, writing in the British Medical Journal in 1976.[iii] He recognised that people “smoke for the nicotine but die from the tar”. Since then, several reports have explored the idea that so long as tobacco is not combusted, nicotine can be consumed at substantially reduced risk. These include the 2001 US Institute of Medicine report Clearing the Smoke: Assessing the Science Base for Tobacco Harm Reduction,[iv] and the UK Royal College of Physicians’ 2007 report Harm reduction in nicotine addiction: helping people who can't quit.[v]
These reports were written before most current safer nicotine products were available (except for snus and NRT). Tobacco harm reduction has been driven both by smokers who want to switch from smoking and the increasing availability of SNP. This switch from smoking has usually occurred without the support of – and sometimes despite opposition from - public health and governments.
Harm reduction and the right to health for all
Harm reduction is a political and social justice issue as well as a public health issue. International treaties make it clear that health is a universal right,[vi] and the UN has accepted that harm reduction for people who use drugs is part of the right to health.[vii] The 1.1 billion people worldwide who smoke have the same right to health as anyone else.
A basic principle of public health endorsed by the World Health Organization is that people should be empowered to have control over their own health in order to live healthier lives.[viii] Tobacco harm reduction is a prime example of people being empowered to take charge of their health by choosing safer ways of using nicotine.
Tobacco harm reduction, the tobacco industry and international tobacco control
Tobacco harm reduction is one of the three pillars of tobacco control. The Framework Convention on Tobacco Control (FCTC)[ix] – the international treaty on tobacco – was enacted in 2005. Its aim was to challenge the increasingly multi-national nature of tobacco companies by bringing nations together to develop measures to control tobacco production and use.[x]
The FCTC states that tobacco control means “a range of supply, demand and harm reduction strategies that aim to improve the health of a population by eliminating or reducing their consumption of tobacco products and exposure to tobacco smoke”. (emphasis added).[xi]
The FCTC does not define harm reduction, but officials drafting the Convention were aware that products might be developed to allow the consumption of nicotine at far less risk to consumers and bystanders. The FCTC also declares that tobacco control measures are dynamic and should be “based on current and relevant scientific, technical and economic considerations”.
The FCTC was enacted before many safer nicotine products were available. The newer SNP were developed and marketed by commercial companies, most of which were not traditional tobacco companies. Vaping products were first developed by the hi-tech electronics industry in China.
Many who have spent years fighting the tobacco industry have wrongly claimed that tobacco harm reduction is merely an industry ruse to lure young people into a lifetime of dependency on nicotine. Alongside these claims, a well-organised and well-funded global campaign has actively sought to undermine the growing evidence base for tobacco harm reduction and its role in helping adult smokers to quit. The campaign has centred on creating a moral panic about (mainly US) young people vaping, despite the fact the US government’s own data show vaping among young people has fallen steeply.[xii] Indeed, in annual surveys carried out by the Centers for Disease Control and Prevention, the number of high school students who reported using e-cigarettes within the past 30 days dropped by 59% between 2019[xiii] and 2021.[xiv] Currently, the WHO opposes tobacco harm reduction, while endorsing a harm reduction approach in many other areas of public health.
What the experts think
An ever-growing body of global independent evidence and reviews from internationally respected professional and medical bodies has stated that safer nicotine products are significantly safer than any combustible, and many types of oral, tobacco products. The evidence shows they have an important role to play in reducing smoking-related death and disease.
International Agency for Research on Cancer: “The use of e-cigarettes is expected to have a lower risk of disease and death than tobacco smoking. […] E-cigarettes have the potential to reduce the enormous burden of disease and death caused by tobacco smoking if most smokers switch to e-cigarettes.”[xv]
The Society for Research on Nicotine and Tobacco leaders: Fifteen past Presidents of the SRNT published a joint statement that “vaping can benefit public health, given substantial evidence supporting the potential of vaping to reduce smoking’s [death] toll. [...] Frequent vaping increases adult smoking cessation [and] completely substituting vaping for smoking likely reduces health risks, possibly substantially.”[xvi]
Public Health England: “Our new review reinforces the finding that vaping is a fraction of the risk of smoking, at least 95% less harmful, and of negligible risk to bystanders. Yet over half of smokers either falsely believe that vaping is as harmful as smoking or just don’t know.”[xvii]
UK Royal College of Physicians: “Although it is not possible to precisely quantify the long-term health risks associated with e-cigarettes, the available data suggest that they are unlikely to exceed 5% of those associated with smoked tobacco products, and may well be substantially lower than this figure. […] E-cigarettes are effective in helping people to stop smoking.”[xviii]
British Medical Association: “Significant numbers of smokers are using e-cigarettes (electronic cigarettes), with many reporting that they are helpful in quitting or cutting down cigarette use. There are clear potential benefits to their use in reducing the substantial harms associated with smoking, and a growing consensus that they are significantly less harmful than tobacco use.”[xix]
New Zealand Ministry of Health: “The Ministry considers vaping products could disrupt inequities and contribute to a Smokefree 2025. The evidence on vaping products indicates they carry much less risk than smoking cigarettes but are not risk-free. Evidence is growing that vaping can help people to quit smoking. There is no international evidence that vaping products are undermining the long-term decline in cigarette smoking among adults and youth and may in fact be contributing to it.”[xx]
Royal Australian College of General Practitioners: “E-cigarettes can relieve cravings and symptoms of nicotine withdrawal as well as simulating the behavioural and sensory aspects of smoking. [...] It is reasonable to conclude that if used as a substitute rather than an addition, e-cigarettes are much less harmful than continuing to smoke.”[xxi]
Cochrane Review: The gold-standard systematic review of randomised controlled trials has concluded that “for every 100 people using nicotine e‐cigarettes to stop smoking, 9 to 14 might successfully stop, compared with only 6 of 100 people using NRT, 7 of 100 using nicotine‐free e‐cigarettes, or four of 100 people having no support or behavioural support only.”[xxii]
US Federal Drug Administration: The FDA has granted a number of Premarket Tobacco Product Applications (PMTAs)[xxiii] and Modified Risk Tobacco Product orders (MRTPs)[xxiv] for safer nicotine products in the US. Approval requires manufacturers to demonstrate the applications are “appropriate for the protection of the public health” with respect to the risks and benefits to the population as a whole. An MRTP authorises the marketing of a tobacco product that poses lower risks compared to other products on the market. General Snus from Swedish Match became the first FDA-approved MRTP in October 2019. In July 2020, the FDA authorized the marketing of PMI’s IQOS heated tobacco product as an MRTP.
Tobacco harm reduction in action
Research carried out by the Global State of Tobacco Harm Reduction estimates that there are 112 million users of safer nicotine products worldwide.[xxv]
The evidence from many countries indicates that smokers are switching to lower risk products. For example, there are clear signs of substitution effects – that SNP are replacing smoking – including in the following countries:
- Norway: 15% of young women use snus but only 1% smoke. It has one of the lowest levels of female smoking in the world and young women use snus rather than cigarettes.[xxvi]
- Japan: Sales of cigarettes have fallen by a third since the introduction of heated tobacco products.[xxvii]
- Sweden: Swedish men have switched from smoking to using snus. As a result, Sweden has the lowest rate of tobacco-related disease in Europe. Sweden is the only EU state to have reached smoke-free status, defined as less than 5% adult smoking prevalence.[xxviii]
- Great Britain: The uptake of vaping has been accompanied by a rapid decline in smoking and vapes are the most popular way to stop smoking. 3.6 million people vape in Great Britain, of whom 2.4 million have completely quit smoking.[xxix]
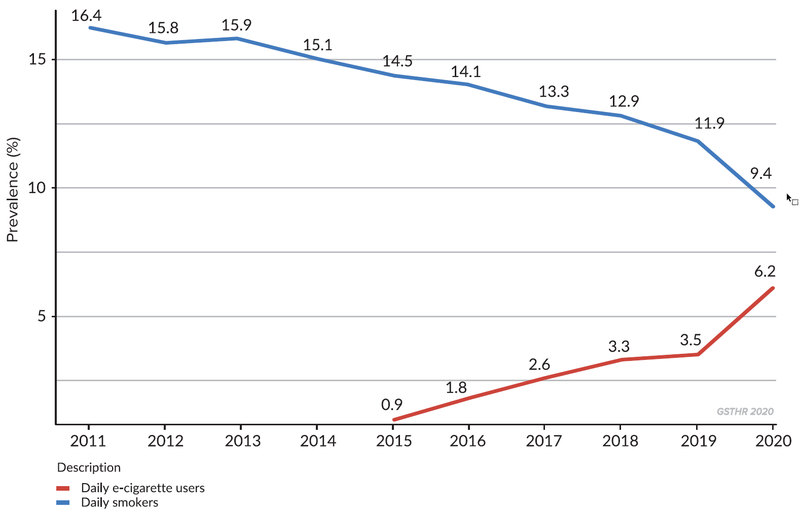
- New Zealand: The rapid uptake of vaping (from 0.9% adults in 2016 to 6.2% in 2021) has been associated with a dramatic fall in smoking – from 14.5% to 9.4%.[xxx]
Changes in smoking and vaping prevalence in New Zealand
What should happen next?
Tobacco harm reduction has a key role to play in the future of tobacco control by reducing global consumption of cigarettes and risky oral tobaccos. It offers new choices to millions of people who want to switch away from smoking and other risky tobacco products. For people who can’t or don’t want to quit nicotine, switching to safer nicotine products offers huge potential benefits.
Governments should facilitate tobacco harm reduction. They should avoid or remove obstacles to the use of safer nicotine products by people who want to quit risky tobacco use. They should implement effective and appropriate regulation that protects consumers and avoids youth uptake. They should also encourage switching among adult smokers and avoid policies and laws that intentionally or unintentionally favour risky products.
For further information about the Global State of Tobacco Harm Reduction’s work, or the points raised in this GSTHR Briefing Paper, please contact [email protected]
About us: Knowledge·Action·Change (K·A·C) promotes harm reduction as a key public health strategy grounded in human rights. The team has over forty years of experience of harm reduction work in drug use, HIV, smoking, sexual health, and prisons. K·A·C runs the Global State of Tobacco Harm Reduction (GSTHR) which maps the development of tobacco harm reduction and the use, availability and regulatory responses to safer nicotine products, as well as smoking prevalence and related mortality, in over 200 countries and regions around the world. For all publications and live data, visit https://gsthr.org
Our funding: The GSTHR project is produced with the help of a grant from the Foundation for a Smoke-Free World, a US non profit 501(c)(3), independent global organization. The project and its outputs are, under the terms of the grant agreement, editorially independent of the Foundation.
[i] Colin D. Mathers and Dejan Loncar, ‘Projections of Global Mortality and Burden of Disease from 2002 to 2030’, PLoS Medicine 3, no. 11 (November 2006): e442, https://doi.org/10.1371/journal.pmed.0030442.
[ii] Royal Society of Public Health – Press release (August 2015) Nicotine “no more harmful to health than caffeine” https://www.rsph.org.uk/about-us/news/nicotine--no-more-harmful-to-health-than-caffeine-.html?s=03
Release accompanies report, Stopping smoking by using other sources of nicotine:
https://www.rsph.org.uk/resourceLibrary/stopping-smoking-by-using-other-sources-of-nicotine.html.
[iii] M A Russell, ‘Low-Tar Medium-Nicotine Cigarettes: A New Approach to Safer Smoking.’, British Medical Journal 1, no. 6023 (12 June 1976): 1430–33.
[iv] Institute of Medicine (US) Committee to Assess the Science Base for Tobacco Harm Reduction, Clearing the Smoke: Assessing the Science Base for Tobacco Harm Reduction, ed. Kathleen Stratton et al. (Washington (DC): National Academies Press (US), 2001), https://www.ncbi.nlm.nih.gov/books/NBK222375/.
[v] Tobacco Advisory Group of the Royal College of Physicians, ‘Harm Reduction in Nicotine Addiction: Helping People Who Can’t Quit’ (London: Royal College of Physicians, October 2007),
[vi] UN Office of the High Commissioner for Human Rights (OHCHR), ‘The Right to Health, Fact Sheet No. 31’ (UN Office of the High Commissioner for Human Rights (OHCHR), June 2008),
https://www.ohchr.org/Documents/Publications/Factsheet31.pdf.
[vii] United Nations, ‘Universal Declaration of Human Rights’, in United Nations (United Nations General Assembly, Paris: United Nations, 1948), https://www.un.org/en/about-us/universal-declaration-of-human-rights.
[viii] World Health Organization, ‘Human Rights and Health’, WHO, 29 December 2017,
https://www.who.int/news-room/fact-sheets/detail/human-rights-and-health.
[ix] WHO, WHO Framework Convention on Tobacco Control (Geneva, Switzerland: World Health Organization, 2005), https://www.who.int/fctc/text_download/en/
[x] Harry Shapiro, ‘Burning Issues: Global State of Tobacco Harm Reduction 2020’ (London: Knowledge-Action-Change, 2020). Chapter 6, page 115:
https://gsthr.org/resources/item/burning-issues-global-state-tobacco-harm-reduction-2020/
[xi] WHO, WHO Framework Convention on Tobacco Control. Article 1 paragraph (d), page 11.
[xii] GSTHR, ‘Fighting the Last War: The WHO and International Tobacco Control’, GSTHR Thematic Reports (London: Knowledge•Action•Change, 2021)
https://gsthr.org/resources/thr-reports/fighting-the-last-war/
GSTHR,‘Fighting the Last War: The WHO and International Tobacco Control’, GSTHR Briefing Papers (London: Knowledge•Action•Change, November 2021)
https://gsthr.org/briefing-papers/fighting-the-last-war-the-who-and-international-tobacco-control/
[xiii] Centers for Disease Control and Prevention - press release, December 2019:
https://www.cdc.gov/media/releases/2019/1205-nyts-2019.html
[xiv] Centers for Disease Control and Prevention, Notes from the Field: E-Cigarette Use Among Middle and High School Students — National Youth Tobacco Survey, United States, 2021
https://www.cdc.gov/mmwr/volumes/70/wr/mm7039a4.htm
[xv] This quote from the WHO agency has since been removed.
[xvi] David J. K. Balfour, et al., Balancing Consideration of the Risks and Benefits of E-Cigarettes, American Journal of Public Health published online September 2021
https://ajph.aphapublications.org/doi/full/10.2105/AJPH.2021.306416
[xvii] Public Health England press release, 6 February 2018:
https://www.gov.uk/government/news/phe-publishes-independent-expert-e-cigarettes-evidence-review
[xviii] Royal College of Physicians, Nicotine without smoke: Tobacco harm reduction https://www.rcplondon.ac.uk/projects/outputs/nicotine-without-smoke-tobacco-harm-reduction
[xix] British Medical Association. E-cigarettes: balancing risks and opportunities. BMA, 2017
https://www.bma.org.uk/media/2083/e-cigarettes-position-paper-v3.pdf
[xx] New Zealand government Position statement on vaping (page updated September 2020):
https://www.health.govt.nz/our-work/preventative-health-wellness/tobacco-control/vaping-smokefree-environments-and-regulated-products/position-statement-vaping
[xxi] The Royal Australian College of General Practitioners, Supporting smoking cessation: a guide for health professionals, 2011 [Updated July 2014]:
https://www.racgp.org.au/download/documents/Guidelines/smoking-cessation.pdf
[xxii] The Cochrane Review. E-cigarettes for smoking cessation. Cochrane, September 2021 (regularly updated).
Plain language summary: https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD010216.pub6/full#CD010216-abs-0002
Full review: https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD010216.pub6/full
[xxiii] U.S. Food and Drug Administration website:
https://www.fda.gov/tobacco-products/premarket-tobacco-product-applications/premarket-tobacco-product-marketing-granted-orders
[xxiv] U.S. Food and Drug Administration website:
https://www.fda.gov/tobacco-products/advertising-and-promotion/modified-risk-granted-orders
[xxv] GSTHR, ‘82 million vapers worldwide in 2021: the GSTHR estimate’, GSTHR Briefing Papers (London: Knowledge•Action•Change, February 2022)
https://gsthr.org/briefing-papers/82-million-vapers-worldwide-in-2021-the-gsthr-estimate/
[xxvi] GSTHR, ‘Fighting the Last War: The WHO and International Tobacco Control’, 2021. Chapter 4, page 29.
https://gsthr.org/resources/thr-reports/fighting-the-last-war/
[xxvii] Ibid.
[xxviii] Ibid.
[xxix] Action on Smoking and Health (ASH) Briefing: Use of e-cigarettes (vapes) among adults in Great Britain (June 2021):
[xxx] Ministry of Health, ‘Annual Data Explorer 2020/21: New Zealand Health Survey [Data File]’, 2021, https://minhealthnz.shinyapps.io/nz-health-survey-2020-21-annual-data-explorer/